Ganglion cysts represent one of the most frequently encountered benign soft tissue masses in orthopaedic and hand surgery practice. These fluid-filled lesions, containing thick synovial fluid resembling clear jelly, commonly develop adjacent to joints and tendons, particularly affecting the wrist, hand, ankle, and foot regions. While many ganglion cysts remain asymptomatic and may resolve spontaneously, others cause significant discomfort, functional impairment, or cosmetic concerns that warrant surgical intervention. Understanding the excision process, recovery expectations, and potential complications enables patients to make informed decisions about their treatment options and prepare adequately for the surgical journey ahead.
Ganglion cyst pathophysiology and anatomical locations
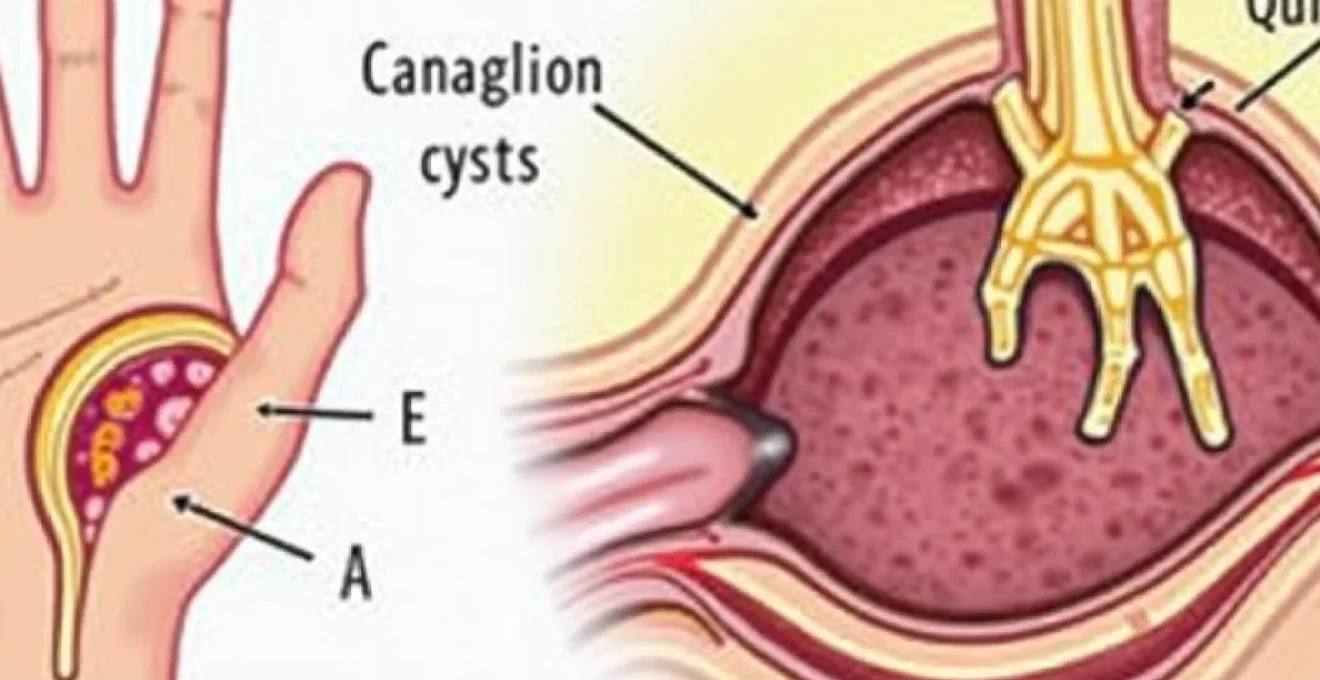
The formation of ganglion cysts involves complex mechanisms related to synovial membrane degeneration and capsular weakening. These benign lesions develop when synovial fluid accumulates within herniated joint capsules or tendon sheaths, creating characteristic smooth, rounded masses beneath the skin. The pathophysiology remains partially understood, with theories suggesting that repetitive microtrauma, joint degeneration, or congenital weakness in capsular structures contribute to their development. Research indicates that ganglion cysts affect women more frequently than men , with peak incidence occurring between ages 20 and 40 years.
Synovial fluid accumulation mechanisms in dorsal wrist ganglions
Dorsal wrist ganglions, comprising approximately 70% of all ganglion cysts, typically originate from the scapholunate ligament region. The accumulation mechanism involves one-way valve systems that allow synovial fluid to flow from the radiocarpal or midcarpal joints into the cyst cavity but prevent backflow. This creates progressive enlargement, particularly during wrist flexion activities that increase intra-articular pressure. The dorsal location makes these cysts highly visible , often causing cosmetic concerns alongside functional limitations. Clinical examination reveals characteristic transillumination properties, where light passes through the cyst contents, distinguishing them from solid masses.
Volar wrist ganglion proximity to radial artery complications
Volar wrist ganglions present unique surgical challenges due to their intimate relationship with critical neurovascular structures, particularly the radial artery. These cysts typically arise from the radiocarpal joint near the scaphoid tubercle, creating potential compression risks for the radial artery and superficial branch of the radial nerve. Surgical excision requires meticulous dissection techniques to avoid iatrogenic injury to these structures. The proximity to major vessels necessitates careful pre-operative planning and may influence the choice between open and arthroscopic techniques. Patients may experience pulsatile sensations or vascular compromise symptoms when large volar ganglions compress surrounding structures.
Flexor tendon sheath ganglia and trigger finger association
Flexor tendon sheath ganglions, also known as seed ganglions or pearl ganglions, develop within the digital flexor tendon sheaths and may contribute to trigger finger pathophysiology. These small, firm masses can mechanically impede tendon gliding, creating catching or locking sensations during finger movement. The association between flexor sheath ganglions and stenosing tenosynovitis requires comprehensive evaluation during surgical planning. Treatment may involve simultaneous tendon sheath release procedures to address both the cyst and underlying triggering mechanism. The compact size and firm consistency of these lesions distinguish them from larger, softer ganglions found elsewhere.
Mucoid cyst formation in distal interphalangeal joints
Mucoid cysts, technically classified as ganglion cysts, develop specifically at distal interphalangeal (DIP) joints in association with underlying osteoarthritis. These lesions contain thick, gelatinous fluid and often communicate with the DIP joint through microscopic channels. The pathophysiology involves osteophyte formation that creates capsular weakness, allowing synovial fluid extravasation. Mucoid cysts frequently cause nail deformities when they compress the nail matrix, creating longitudinal grooves or ridging. Surgical management often requires simultaneous osteophyte removal to address the underlying degenerative process and reduce recurrence risk.
Pre-operative assessment and diagnostic imaging protocols
Comprehensive pre-operative evaluation forms the foundation of successful ganglion cyst management, involving detailed clinical examination, patient history assessment, and appropriate diagnostic imaging studies. The evaluation process begins with thorough questioning about symptom onset, pain characteristics, functional limitations, and previous treatment attempts. Physical examination techniques include palpation for consistency, mobility, transillumination testing, and assessment of surrounding neurovascular structures. Accurate diagnosis ensures appropriate treatment selection and helps identify potential complications that may influence surgical approach or anaesthetic choice.
High-resolution ultrasound evaluation for ganglion characterisation
High-resolution ultrasound provides excellent visualisation of ganglion cysts, offering real-time assessment of cyst characteristics, joint communication, and surrounding soft tissue relationships. Modern ultrasound equipment with high-frequency probes (12-18 MHz) delivers superior image quality for superficial structures, enabling detailed evaluation of cyst wall thickness, internal echo patterns, and vascularity. Ultrasound guidance facilitates accurate aspiration procedures when conservative treatment is attempted before surgical intervention. The dynamic nature of ultrasound examination allows assessment of cyst behaviour during joint movement, helping identify connections to underlying joints or tendon sheaths that may influence surgical planning.
MRI T2-Weighted imaging for occult ganglion detection
Magnetic resonance imaging, particularly T2-weighted sequences, provides superior soft tissue contrast for detecting occult ganglions that may not be clinically apparent. MRI demonstrates characteristic high signal intensity on T2-weighted images, reflecting the high water content of synovial fluid within the cyst. Advanced MRI techniques can reveal joint communications and identify multiple cysts that might be missed during clinical examination. The multiplanar imaging capability of MRI assists surgical planning by demonstrating anatomical relationships with critical structures, particularly important for complex cases involving deep-seated or recurrent ganglions.
Aspiration cytology techniques using 18-gauge needles
Diagnostic aspiration using 18-gauge needles provides both therapeutic and diagnostic benefits, allowing cytological examination of cyst contents while potentially providing symptom relief. The procedure involves sterile preparation, local anaesthetic infiltration, and careful needle insertion guided by palpation or ultrasound visualisation. Cytological analysis confirms the diagnosis by demonstrating characteristic findings including mucin-rich fluid with scattered inflammatory cells and absence of malignant features. The thick, viscous nature of ganglion contents may require larger gauge needles or multiple attempts to obtain adequate samples for analysis.
Differential diagnosis from giant cell tumours and lipomas
Accurate differential diagnosis distinguishes ganglion cysts from other soft tissue masses, including giant cell tumours of tendon sheath, lipomas, and synovial sarcomas. Giant cell tumours typically present as firm, non-transilluminable masses with characteristic MRI findings showing low signal intensity on T2-weighted images. Lipomas demonstrate characteristic fatty signal intensity on MRI sequences and lack the fluid characteristics of ganglion cysts. Synovial sarcomas, though rare, require careful consideration in atypical presentations or rapidly growing masses. The combination of clinical presentation, imaging findings, and aspiration cytology usually provides definitive diagnosis, though histopathological examination following excision confirms the diagnosis and rules out malignancy.
Surgical excision techniques and procedural approaches
Surgical excision represents the most definitive treatment for symptomatic ganglion cysts, offering superior recurrence rates compared to aspiration techniques. The choice between open and arthroscopic approaches depends on cyst location, size, surgeon expertise, and patient factors. Modern surgical techniques emphasise complete excision of the cyst along with its stalk or communication to the parent joint, reducing recurrence risk. Patient positioning, anaesthetic selection, and surgical instrument preparation require careful consideration to optimise outcomes and minimise complications.
Open excision under local anaesthesia with lidocaine infiltration
Open excision under local anaesthesia provides excellent visualisation and control for most ganglion cyst procedures, particularly suitable for superficial lesions in cooperative patients. The technique involves infiltration with lidocaine containing epinephrine to provide anaesthesia and haemostasis. Local anaesthesia offers several advantages including reduced systemic risks, faster recovery, and cost-effectiveness compared to general anaesthesia. The procedure begins with sterile preparation and draping, followed by careful marking of the incision line over the cyst. Dissection proceeds through skin and subcutaneous tissues, identifying and protecting surrounding structures while isolating the cyst and its connections.
Arthroscopic ganglion resection using 2.7mm arthroscopes
Arthroscopic techniques utilise small-diameter arthroscopes (2.7mm) to visualise and excise ganglion cysts through minimally invasive portals. This approach proves particularly valuable for dorsal wrist ganglions with clear joint communication, allowing simultaneous evaluation and treatment of intra-articular pathology. Arthroscopic resection offers reduced scarring and potentially faster recovery compared to open techniques, though it requires specialised equipment and expertise. The procedure involves standard arthroscopic portal placement, joint distension with saline, and systematic identification of the ganglion stalk origin. Electrocautery or mechanical shavers facilitate complete excision while maintaining clear visualisation throughout the procedure.
Capsular repair following dorsal wrist ganglion removal
Complete excision of dorsal wrist ganglions often requires removal of a portion of the joint capsule at the stalk origin, necessitating careful capsular repair to prevent recurrence and maintain joint stability. The repair technique involves identifying viable capsular edges and approximating them with absorbable sutures. Proper capsular repair reduces recurrence risk by eliminating the pathway for future synovial fluid accumulation. The repair must balance adequate closure with preservation of joint mobility, avoiding over-tightening that could restrict wrist motion. Some surgeons advocate for imbrication techniques that reinforce the repair while addressing any underlying capsular laxity.
Tourniquet application and bloodless field maintenance
Tourniquet application creates a bloodless surgical field, enhancing visualisation and precision during ganglion excision procedures. Standard techniques involve appropriate cuff sizing, limb exsanguination using elastic bandages or pneumatic devices, and maintenance of adequate pressure throughout the procedure. Bloodless conditions facilitate identification of small structures and ensure complete cyst excision without bleeding obscuring the operative field. Tourniquet time should be monitored and documented, with most procedures completed well within safe time limits. Post-operative tourniquet release allows assessment of haemostasis and identification of any bleeding points requiring attention.
Microscopic examination of excised ganglion wall tissue
Histopathological examination of excised ganglion tissue provides definitive diagnosis and rules out malignancy, though routine examination is not always necessary for typical presentations. Microscopic features include a fibrous wall lacking true epithelial lining, with surrounding connective tissue showing myxoid degeneration. The absence of epithelial lining distinguishes ganglions from true cysts , supporting the theory that they represent herniations rather than true cystic lesions. Special stains may highlight mucin content and inflammatory infiltrates, while immunohistochemical studies can exclude other soft tissue lesions when diagnostic uncertainty exists.
Post-operative recovery timeline and rehabilitation protocols
Recovery following ganglion cyst excision typically progresses through predictable phases, with most patients experiencing significant improvement within 4-6 weeks. The initial post-operative period focuses on wound healing, pain management, and gradual mobilisation to prevent stiffness while protecting the surgical site. Early mobilisation within comfort limits helps prevent adhesions and maintains joint function, though specific protocols vary based on cyst location and surgical technique employed. Patient education regarding expected recovery milestones, activity restrictions, and warning signs helps optimise outcomes and reduce anxiety during the healing process.
The first 48-72 hours involve management of post-operative pain and swelling, with elevation and ice application providing symptomatic relief. Dressing changes typically begin 24-48 hours post-operatively, allowing wound inspection and early detection of complications such as infection or excessive swelling. Pain levels generally peak within the first 24 hours and gradually subside over the subsequent week, with most patients transitioning from prescription analgesics to over-the-counter medications by day 3-5. Suture removal occurs at 10-14 days, depending on wound healing progress and suture type used.
Week 2-4 marks the transition to more active rehabilitation, with emphasis on range of motion exercises and gradual return to activities of daily living. Physical therapy referral may be appropriate for patients experiencing significant stiffness or those with occupational demands requiring specific functional restoration. Return to work timing varies considerably based on job requirements, with office workers typically resuming duties within 1-2 weeks while manual labourers may require 4-6 weeks for full activity clearance. Driving restrictions depend on surgical site location and individual comfort levels, with most patients cleared for driving once they can safely operate controls without pain or restriction.
Potential complications and risk management strategies
While ganglion cyst excision generally carries low complication rates, understanding potential risks enables appropriate prevention strategies and early recognition of problems. Common complications include wound healing issues, infection, nerve injury, stiffness, and recurrence, each requiring specific management approaches. Comprehensive pre-operative counselling helps patients understand realistic expectations and participate actively in risk reduction through proper post-operative care compliance.
Infection rates remain low (typically <2%) but require prompt recognition and treatment to prevent serious complications. Risk factors include diabetes, immunosuppression, smoking, and inadequate wound care, with prevention strategies focusing on sterile technique, prophylactic antibiotics when indicated, and patient education regarding proper wound hygiene. Early signs of infection include increasing pain, redness, warmth, and drainage , necessitating immediate medical evaluation and potential antibiotic therapy. Deep infections may require surgical drainage and debridement, though such complications remain rare with proper technique and care.
Nerve injury represents a potentially serious complication, particularly relevant for volar wrist ganglions near the radial nerve or digital ganglions affecting digital nerves. Prevention involves careful anatomical dissection, adequate exposure, and identification of nerve structures before proceeding with excision. Temporary numbness may occur due to surgical manipulation or swelling, typically resolving over several weeks to months. Permanent nerve injury resulting in persistent numbness or dysaesthesias occurs rarely but may require additional treatment including nerve repair or neuroma excision in severe cases.
Recurrence rates following complete surgical excision range from 5-15%, significantly lower than aspiration techniques which demonstrate recurrence rates of 50-85%.
Long-term outcomes and recurrence prevention methods
Long-term outcomes following ganglion cyst excision are generally excellent, with most patients experiencing complete symptom resolution and return to normal activities. Studies demonstrate satisfaction rates exceeding 90% at long-term follow-up, with significant improvements in pain, function, and cosmetic appearance. Success rates correlate strongly with complete excision of the cyst and its communication to the parent joint, emphasising the importance of thorough surgical technique during the initial procedure.
Recurrence prevention strategies focus on complete surgical excision, proper post-operative care, and identification of predisposing factors that may contribute to cyst reformation. Incomplete excision, particularly failure to address the stalk or communication site, represents the primary risk factor for recurrence. Arthroscopic techniques may offer advantages in visualising and completely excising the stalk origin, though both open and arthroscopic approaches can achieve excellent results with proper technique. Patient factors including repetitive activities, underlying arthritis, or genetic predisposition may influence recurrence risk and require ongoing monitoring.
Follow-up protocols typically include clinical examination at 2-3 weeks, 6 weeks, and 3 months post-operatively, with additional visits as needed based on recovery progress. Long-term surveillance may be appropriate for patients at higher recurrence risk or those with occupational exposures predisposing to cyst formation. Patient education regarding activity modification and ergonomic principles helps reduce repetitive
trauma and reduce long-term recurrence rates. Regular communication with healthcare providers helps identify any concerning changes early, enabling prompt intervention if complications arise.
Functional outcomes demonstrate consistent improvements across multiple domains, with objective measurements showing restored grip strength, improved range of motion, and enhanced dexterity following recovery. Return to sports and recreational activities typically occurs within 6-8 weeks, though contact sports may require additional protection during initial return phases. Quality of life measurements consistently improve following successful ganglion excision, with patients reporting decreased anxiety about appearance, reduced activity limitations, and improved sleep quality when pre-operative pain resolves.
Prevention strategies extend beyond surgical technique to include lifestyle modifications and occupational considerations that may reduce future cyst development. Ergonomic workplace assessments help identify repetitive stress factors contributing to ganglion formation, while activity modification counselling provides patients with tools to reduce recurrence risk. Maintaining joint flexibility through regular stretching and avoiding prolonged static positioning may help prevent the capsular changes that predispose to ganglion development, though genetic factors remain beyond patient control.