Sinus-related toothaches represent one of the most misunderstood forms of dental pain, often leading patients down a frustrating path of unnecessary dental treatments when the root cause lies within their nasal cavities. The intimate anatomical relationship between the maxillary sinuses and upper tooth roots creates a complex pain referral pattern that can mimic genuine dental pathology. When sinusitis develops, the resulting inflammation and pressure buildup can trigger intense pain signals that patients experience as authentic toothache, particularly affecting the posterior maxillary teeth.
Understanding this connection proves crucial for both patients and healthcare providers, as proper diagnosis determines treatment success . The maxillary sinuses, positioned directly above the roots of upper premolars and molars, can exert significant pressure on dental nerve endings when inflamed or infected. This phenomenon affects millions of individuals annually, with sinus-related dental pain accounting for approximately 15-20% of all reported toothaches in clinical practice.
Maxillary sinus anatomy and its connection to upper molar root systems
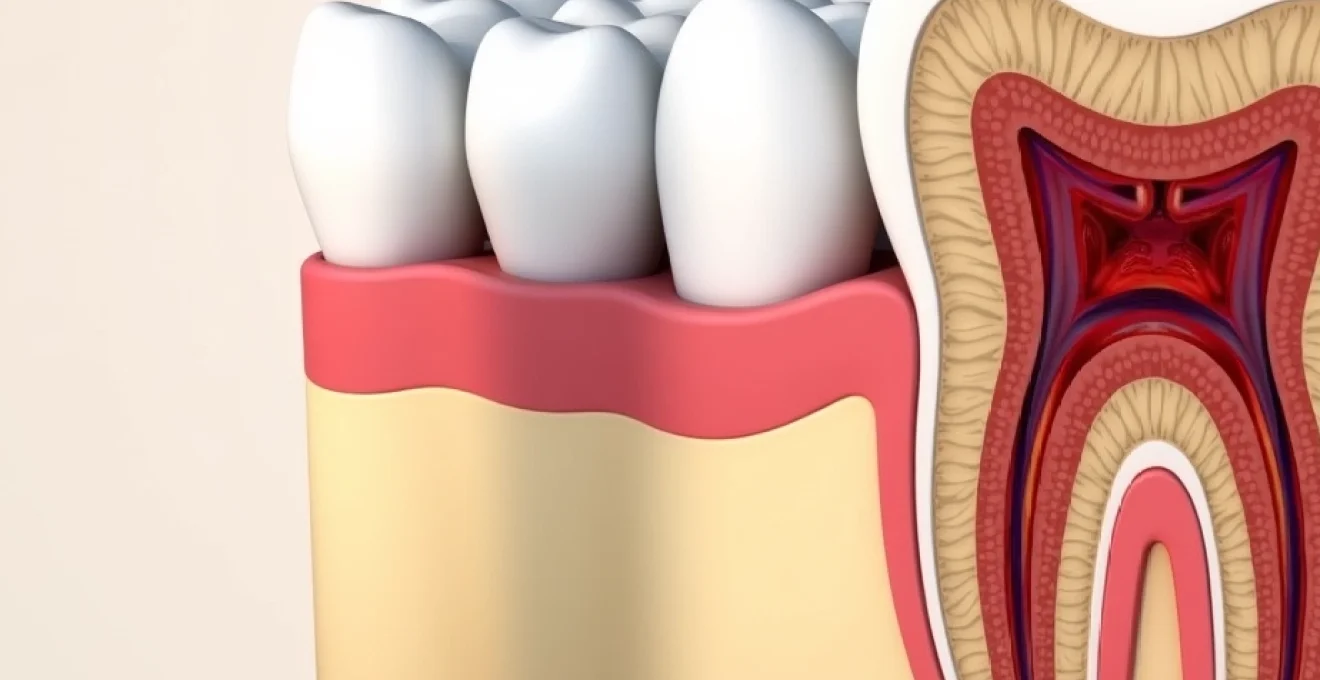
The maxillary sinuses, also known as the antra of Highmore, represent the largest of the paranasal air spaces and maintain an intricate anatomical relationship with the upper dentition. These pyramid-shaped cavities extend from the nasal cavity laterally, with their floor positioned remarkably close to the alveolar process housing the maxillary teeth. In many individuals, particularly those with extensive pneumatisation, the sinus floor may extend between or even below the apices of the posterior teeth, creating a direct pathway for inflammatory processes to affect dental structures.
The proximity between sinus anatomy and dental roots varies significantly among individuals, with studies indicating that approximately 60-70% of people demonstrate some degree of maxillary sinus floor depression around the root apices. This anatomical variation explains why some patients experience severe dental pain during sinus infections whilst others remain relatively comfortable. The thickness of bone separating the sinus floor from tooth roots often measures less than 1-2 millimetres, and in some cases, the roots may actually project into the sinus cavity itself, covered only by the delicate Schneiderian membrane.
Zygomatic process and alveolar ridge proximity to sinus floor
The zygomatic process forms the lateral and superior boundaries of the maxillary sinus, whilst the alveolar ridge creates the inferior border. This architectural arrangement places the first and second maxillary molars in particularly vulnerable positions, as their roots frequently extend closest to or into the sinus cavity. Radiographic studies reveal that the mesial roots of maxillary first molars demonstrate the highest incidence of sinus floor proximity, followed closely by the second molar roots.
The palatal roots of maxillary molars tend to maintain greater distance from the sinus floor compared to their buccal counterparts, though individual anatomical variations can significantly alter this pattern. Understanding these relationships proves essential when evaluating patients presenting with posterior maxillary tooth pain, as the location and character of discomfort often correlate with specific anatomical configurations.
Periodontal ligament inflammation pathways through schneiderian membrane
The Schneiderian membrane, a thin pseudostratified ciliated epithelium lining the maxillary sinus, serves as both a protective barrier and a potential pathway for inflammatory mediator transmission. When sinusitis develops, inflammatory cytokines and bacterial toxins can penetrate this membrane, affecting the periodontal ligament spaces of adjacent teeth. This process creates a phenomenon known as sympathetic dental pain , where perfectly healthy teeth become exquisitely sensitive due to secondary inflammation.
Research has demonstrated that certain inflammatory molecules, particularly prostaglandin E2 and interleukin-1β, can traverse the thin bone-membrane interface and stimulate nociceptors within the periodontal ligament. This mechanism explains why patients with acute maxillary sinusitis frequently report throbbing, pressure-like sensations in multiple posterior teeth simultaneously, rather than the sharp, localised pain typical of dental caries or pulpitis.
Trigeminal nerve branch distribution in maxillary sinusitis cases
The maxillary division of the trigeminal nerve (cranial nerve V2) provides sensory innervation to both the maxillary sinus mucosa and the posterior maxillary teeth through its superior alveolar nerve branches. This shared innervation pathway creates the neurological basis for sinus-related tooth pain, as inflammatory processes affecting the sinus lining can trigger pain signals that the brain interprets as originating from dental structures.
The posterior superior alveolar nerve, which supplies the maxillary molars, travels through the posterior wall of the maxillary sinus before entering the alveolar canals. During acute sinusitis, inflammation and oedema surrounding these nerve pathways can compress or irritate the nerve fibres, producing the characteristic deep, aching sensation that patients describe as toothache. This explains why conventional dental anaesthesia may provide only temporary relief for sinus-related dental pain.
Radiographic evidence of apical root extension into antral space
Modern radiographic techniques, particularly cone beam computed tomography (CBCT), have revolutionised our understanding of maxillary sinus-tooth relationships. These high-resolution images frequently reveal root apices extending directly into the sinus cavity, with only the thin Schneiderian membrane providing separation from the air space. Such findings are particularly common in the maxillary first and second molars, where up to 35% of cases demonstrate some degree of root protrusion into the antrum.
Conventional panoramic radiographs may underestimate the true extent of sinus-root proximity due to their two-dimensional nature and inherent magnification factors. CBCT imaging provides three-dimensional visualisation that allows precise measurement of bone thickness between root apices and sinus floor, enabling clinicians to predict which patients may be most susceptible to sinus-related dental symptoms during upper respiratory infections.
Differential diagnosis between odontogenic and rhinogenic sinus pain
Distinguishing between genuine dental pathology and sinus-related tooth pain requires a systematic diagnostic approach that considers both dental and sinonasal factors. The challenge lies in the fact that both conditions can produce remarkably similar symptoms, including temperature sensitivity, pressure sensation, and throbbing discomfort. However, several key distinguishing features can guide clinicians toward the correct diagnosis and appropriate treatment pathway.
Timing represents one of the most significant diagnostic clues, as sinus-related dental pain typically follows or accompanies upper respiratory symptoms such as nasal congestion, rhinorrhoea, or facial pressure. Patients often report that their tooth pain began several days after developing cold-like symptoms, in contrast to odontogenic pain which usually develops independently of respiratory illness. The bilateral nature of sinus-related discomfort also differs markedly from typical dental pain, which tends to be unilateral and precisely localised to a specific tooth.
Percussion testing techniques for maxillary premolars and molars
Percussion testing remains a fundamental component of dental diagnosis, though its interpretation requires modification when evaluating suspected sinus-related pain. Traditional vertical percussion may elicit discomfort in both odontogenic and rhinogenic cases, making differentiation challenging. However, the pattern and quality of percussion response can provide valuable diagnostic information when properly evaluated.
In cases of sinus-related tooth pain, percussion typically produces a dull, diffuse sensation across multiple teeth rather than the sharp, localised response characteristic of apical periodontitis. Additionally, the percussion response in sinus cases often varies with head position, becoming more pronounced when the patient bends forward or assumes a dependent head position, reflecting changes in sinus pressure and fluid dynamics.
Cold stimulus response patterns in Sinus-Related dental pain
Thermal testing provides another crucial diagnostic tool for differentiating sinus-related from odontogenic tooth pain. Healthy teeth affected by sinus pressure typically maintain normal responses to cold stimulation, producing brief, sharp sensations that subside quickly once the stimulus is removed. This contrasts sharply with the prolonged, intense responses seen in cases of irreversible pulpitis or the absent responses characteristic of pulpal necrosis.
The application of cold testing should be systematic, evaluating each posterior maxillary tooth individually whilst noting the duration and intensity of response. Patients with sinus-related discomfort often report that cold application provides temporary relief by numbing the area, whereas those with genuine pulpal pathology typically experience increased pain intensity with thermal stimulation.
Orthopantomogram interpretation for sinus floor pathology
Panoramic radiographs offer valuable insights into maxillary sinus health and its relationship to dental structures, though interpretation requires understanding of the technique’s limitations and normal anatomical variations. The sinus floors should appear as radiopaque lines with relatively uniform thickness and smooth contours. Areas of thickening, discontinuity, or haziness may indicate inflammatory changes affecting the sinus lining.
Mucosal thickening appears as radiopaque bands along the sinus floor and walls, often accompanied by loss of the normal air-filled radiolucency within the sinus cavity. Studies suggest that mucosal thickening exceeding 2-3 millimetres correlates with clinically significant sinusitis, though correlation with symptoms remains more important than absolute measurements . Complete opacification of the sinus cavity indicates severe inflammation or possible fluid accumulation requiring medical intervention.
Nasal endoscopy findings in secondary maxillary sinusitis
Nasal endoscopy performed by ENT specialists can provide direct visualisation of the sinonasal anatomy and identify specific pathological changes contributing to maxillary sinusitis. Key findings include mucosal oedema, purulent discharge from the middle meatus, and anatomical abnormalities such as deviated nasal septum or enlarged turbinates that may impede normal sinus drainage.
The presence of purulent drainage specifically from the maxillary sinus outflow tract strongly supports the diagnosis of bacterial sinusitis and may guide antibiotic selection. Endoscopic examination also allows assessment of the ostiomeatal complex, the critical drainage pathway for the maxillary sinus, helping identify structural factors that may predispose to recurrent infections.
Pharmacological management using targeted Anti-Inflammatory protocols
Effective pharmacological management of sinus-related toothache requires a multi-modal approach targeting both the underlying sinusitis and the secondary dental pain. The primary therapeutic goal involves reducing sinus inflammation and promoting drainage, which subsequently relieves pressure on dental nerve endings and resolves the referred pain. Non-steroidal anti-inflammatory drugs (NSAIDs) form the cornerstone of treatment, providing both analgesic and anti-inflammatory effects that address multiple aspects of the condition.
Ibuprofen represents the preferred NSAID for sinus-related dental pain, with typical dosing of 400-600mg every 6-8 hours providing optimal anti-inflammatory effects. This dosage schedule maintains therapeutic blood levels whilst minimising gastrointestinal side effects. For patients unable to tolerate NSAIDs, paracetamol 500-1000mg every 6 hours offers analgesic benefits, though it lacks the anti-inflammatory properties crucial for addressing sinus mucosal swelling.
Topical nasal corticosteroids such as fluticasone or mometasone demonstrate excellent efficacy in reducing sinus inflammation and promoting mucociliary clearance. These medications require 2-3 days to achieve peak effectiveness but provide sustained anti-inflammatory effects with minimal systemic absorption. Proper application technique proves crucial for optimal outcomes , with patients requiring instruction on correct spray positioning and timing to ensure adequate medication deposition on inflamed sinus tissues.
Research indicates that combining oral NSAIDs with topical corticosteroids produces superior outcomes compared to either treatment alone, with 78% of patients experiencing significant symptom improvement within 5-7 days of initiation.
Decongestants offer additional therapeutic benefits by reducing mucosal swelling and improving sinus ventilation. Oral formulations such as pseudoephedrine 60mg every 6 hours provide systemic decongestant effects, though usage should be limited to 3-5 days to avoid rebound congestion. Topical decongestant sprays containing oxymetazoline or xylometazoline offer rapid onset of action but carry higher risk of rhinitis medicamentosa with prolonged use.
Nasal irrigation systems and mucociliary clearance enhancement
Nasal irrigation represents one of the most effective non-pharmacological interventions for sinus-related tooth pain, working by mechanically removing inflammatory debris, reducing bacterial load, and promoting normal mucociliary function. The technique involves introducing isotonic saline solution into the nasal cavity under controlled pressure, allowing gravity and hydraulic flow to flush secretions from the sinuses and nasal passages.
Various irrigation systems are available, ranging from simple squeeze bottles to sophisticated pulsatile devices. The neti pot remains the most widely recognised method, utilising gravity flow to deliver saline solution through one nostril whilst allowing drainage through the opposite side. More advanced systems employ positive pressure delivery, which may provide superior penetration into sinus cavities but requires proper technique to avoid complications such as middle ear pressure changes.
The composition of irrigation solutions significantly influences therapeutic outcomes. Standard isotonic saline (0.9% sodium chloride) provides effective cleansing with minimal mucosal irritation. Some practitioners advocate for slightly hypertonic solutions (1.5-3% saline) to enhance osmotic removal of oedema fluid from inflamed tissues, though these concentrations may cause temporary burning sensations. Adding sodium bicarbonate (baking soda) creates a buffered solution that reduces irritation and may enhance mucolytic effects on thick secretions.
Frequency and timing of irrigation sessions impact effectiveness significantly. Acute sinusitis typically responds to 2-3 daily irrigation sessions, with morning treatments particularly beneficial for clearing overnight accumulations. Each session should involve 100-250ml of solution per nostril, delivered slowly to allow adequate contact time with inflamed tissues. Patients should be advised that initial treatments may temporarily increase nasal congestion as loosened secretions are mobilised.
Temperature considerations prove important for patient comfort and therapeutic efficacy. Body-temperature solutions (37°C) provide optimal comfort and avoid triggering vasomotor responses that could worsen congestion. Solutions that are too hot may damage delicate nasal tissues, whilst cold irrigants can stimulate increased mucus production and vasoconstriction that impedes drainage.
Advanced treatment modalities for chronic maxillary sinusitis
When conventional treatments fail to provide adequate relief for chronic maxillary sinusitis and associated dental pain, advanced therapeutic modalities may be necessary to restore normal sinus function and eliminate symptoms. These interventions typically require specialist evaluation and may involve both medical and surgical approaches tailored to individual anatomical and pathological factors.
Balloon sinuplasty has emerged as a minimally invasive surgical option for patients with chronic sinusitis refractory to medical management. This technique involves introducing a small balloon catheter through the natural sinus ostium, then inflating it to dilate the opening and restore normal drainage pathways. Studies demonstrate success rates of 85-90% for symptom improvement, with significantly shorter recovery times compared to traditional functional endoscopic sinus surgery (FESS).
Culture-directed antibiotic therapy may be necessary for cases involving resistant bacterial organisms or biofilm formation. Endoscopically guided cultures obtained directly from the maxillary sinus provide more accurate organism identification compared to nasal swabs, allowing targeted antimicrobial selection. Extended antibiotic courses of 3-4 weeks may be required to penetrate biofilms and achieve bacterial eradication, particularly in cases involving Staphylococcus aureus or Pseudomonas aeruginosa .
Antifungal therapy assumes increasing importance as awareness of fungal sinusitis grows. Allergic fungal sinusitis, characterised by eosinophilic mucin and fungal hyphae within sinonasal secretions, requires systemic corticosteroids combined with antifungal medications such as itraconazole or voriconazole. This condition often presents with severe facial pain and pressure that can mimic dental pathology, making proper diagnosis crucial for treatment success.
Advanced imaging techniques, including MRI with gadolinium contrast, can identify fungal sinusitis patterns that appear as characteristic signal changes on T1 and T2-weighted sequences, helping guide appropriate antifungal therapy selection.
Immunomodulatory treatments represent emerging therapeutic options for patients with chronic rhinosinusitis and concurrent dental symptoms. Low-dose macrolide antibiotics such as clarithromycin or azithromycin, administered for their anti-inflammatory rather than antimicrobial properties, demonstrate efficacy in reducing sinus inflammation and improving mucociliary clear
ance. These medications work by modulating cytokine production and reducing neutrophil recruitment to inflamed tissues, potentially breaking the cycle of chronic inflammation that perpetuates both sinus disease and associated dental symptoms.
Post-treatment monitoring and recurrence prevention strategies
Successful management of sinus-related toothache extends beyond initial symptom resolution to encompass comprehensive monitoring protocols and prevention strategies that address underlying predisposing factors. Regular follow-up assessments allow clinicians to evaluate treatment effectiveness, identify early signs of recurrence, and modify therapeutic approaches based on patient response patterns. The multifaceted nature of chronic rhinosinusitis requires ongoing surveillance to prevent progression and maintain long-term symptom control.
Patient education forms the cornerstone of recurrence prevention, empowering individuals to recognise early warning signs and implement appropriate interventions before symptoms escalate. Key educational components include instruction on proper nasal hygiene techniques, environmental modification strategies, and understanding of trigger factors that may precipitate sinus inflammation. Patients should be taught to monitor for subtle changes in nasal discharge, facial pressure, or dental sensitivity that may herald impending flare-ups.
Environmental control measures prove particularly crucial for patients with allergic components to their sinus disease. Indoor air quality management involves maintaining humidity levels between 30-50%, regular cleaning of air conditioning systems, and implementation of HEPA filtration where appropriate. Allergen avoidance strategies should be tailored to individual sensitivities identified through skin testing or specific IgE measurements, with particular attention to dust mites, mould spores, and seasonal pollens that commonly trigger sinonasal inflammation.
Long-term maintenance therapy may be necessary for patients with recurrent episodes of sinus-related dental pain. Low-dose topical corticosteroids used 2-3 times weekly can help maintain mucosal health and prevent inflammatory flare-ups without significant systemic absorption. Some patients benefit from prophylactic nasal irrigation during high-risk periods such as seasonal pollen exposure or upper respiratory infection outbreaks, helping to maintain optimal mucociliary clearance function.
Clinical studies demonstrate that patients who maintain regular nasal hygiene routines experience 60% fewer episodes of acute sinusitis compared to those who discontinue preventive measures after symptom resolution.
Dental considerations in post-treatment monitoring include regular evaluation of posterior maxillary teeth for signs of secondary dental pathology that may develop following prolonged sinus inflammation. The chronic inflammatory environment can potentially affect tooth vitality over time, particularly in cases where root apices extend into the sinus cavity. Routine dental examinations should include thermal testing and radiographic assessment to detect early pulpal changes that might require intervention.
Documentation of treatment responses and trigger patterns enables personalised management strategies that can significantly reduce recurrence rates. Patients should maintain symptom diaries noting environmental exposures, dietary factors, stress levels, and medication compliance to identify patterns that may guide future therapeutic decisions. This information proves invaluable for adjusting treatment protocols and implementing targeted prevention measures based on individual risk factors and response patterns.
The integration of dental and medical care ensures comprehensive management that addresses both the immediate symptoms and underlying anatomical or physiological factors contributing to recurrent episodes. Regular communication between dental and medical providers facilitates coordinated care approaches that optimise outcomes whilst avoiding duplication of treatments or conflicting therapeutic recommendations that could compromise patient safety and treatment effectiveness.